
Synopsis
0
CEP/COS
0
JDMF
0
KDMF
0
NDC API
0
VMF
0
FDA Orange Book

0
Canada

DRUG PRODUCT COMPOSITIONS
0
API
0
FDF
0
Data Compilation #PharmaFlow
0
Stock Recap #PipelineProspector
0
Weekly News Recap #Phispers
API SUPPLIERS
 FULL SCREEN VIEW Click here to open all results in a new tab [this preview display 10 results]
FULL SCREEN VIEW Click here to open all results in a new tab [this preview display 10 results]
USDMF
FULL SCREEN VIEW Click here to open all results in a new tab [this preview display 10 results]EU WC
FULL SCREEN VIEW Click here to open all results in a new tab [this preview display 10 results]Listed Suppliers
FULL SCREEN VIEW Click here to open all results in a new tab [this preview display 10 results]API Reference Price

API/FDF Prices: Book a Demo to explore the features and consider upgrading later
API Imports and Exports
INTERMEDIATE SUPPLIERS
FULL SCREEN VIEW Click here to open all results in a new tab [this preview display 10 results]FDF Dossiers
FULL SCREEN VIEW Click here to open all results in a new tab [this preview display 10 results]Europe
FULL SCREEN VIEW Click here to open all results in a new tab [this preview display 10 results]Australia
FULL SCREEN VIEW Click here to open all results in a new tab [this preview display 10 results]Digital Content ![]()

NEWS #PharmaBuzz
Global Sales Information
REF. STANDARDS & IMPURITIES
ABOUT THIS PAGE
72
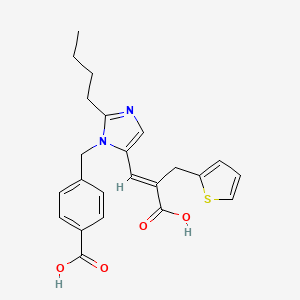
PharmaCompass offers a list of Eprosartan API manufacturers, exporters & distributors, which can be sorted by GMP, USDMF, JDMF, KDMF, CEP (COS), WC, Price,and more, enabling you to easily find the right Eprosartan manufacturer or Eprosartan supplier for your needs.
Send us enquiries for free, and we will assist you in establishing a direct connection with your preferred Eprosartan manufacturer or Eprosartan supplier.
PharmaCompass also assists you with knowing the Eprosartan API Price utilized in the formulation of products. Eprosartan API Price is not always fixed or binding as the Eprosartan Price is obtained through a variety of data sources. The Eprosartan Price can also vary due to multiple factors, including market conditions, regulatory modifications, or negotiated pricing deals.
A Eprosartan manufacturer is defined as any person or entity involved in the manufacture, preparation, processing, compounding or propagation of Eprosartan, including repackagers and relabelers. The FDA regulates Eprosartan manufacturers to ensure that their products comply with relevant laws and regulations and are safe and effective to use. Eprosartan API Manufacturers are required to adhere to Good Manufacturing Practices (GMP) to ensure that their products are consistently manufactured to meet established quality criteria.
click here to find a list of Eprosartan manufacturers with USDMF, JDMF, KDMF, CEP, GMP, COA and API Price related information on PhamaCompass.
A Eprosartan supplier is an individual or a company that provides Eprosartan active pharmaceutical ingredient (API) or Eprosartan finished formulations upon request. The Eprosartan suppliers may include Eprosartan API manufacturers, exporters, distributors and traders.
click here to find a list of Eprosartan suppliers with USDMF, JDMF, KDMF, CEP, GMP, COA and API Price related information on PharmaCompass.
A Eprosartan DMF (Drug Master File) is a document detailing the whole manufacturing process of Eprosartan active pharmaceutical ingredient (API) in detail. Different forms of Eprosartan DMFs exist exist since differing nations have different regulations, such as Eprosartan USDMF, ASMF (EDMF), JDMF, CDMF, etc.
A Eprosartan DMF submitted to regulatory agencies in the US is known as a USDMF. Eprosartan USDMF includes data on Eprosartan's chemical properties, information on the facilities and procedures used, and details about packaging and storage. The Eprosartan USDMF is kept confidential to protect the manufacturer’s intellectual property.
click here to find a list of Eprosartan suppliers with USDMF on PharmaCompass.
A Eprosartan written confirmation (Eprosartan WC) is an official document issued by a regulatory agency to a Eprosartan manufacturer, verifying that the manufacturing facility of a Eprosartan active pharmaceutical ingredient (API) adheres to the Good Manufacturing Practices (GMP) regulations of the importing country. When exporting Eprosartan APIs or Eprosartan finished pharmaceutical products to another nation, regulatory agencies frequently require a Eprosartan WC (written confirmation) as part of the regulatory process.
click here to find a list of Eprosartan suppliers with Written Confirmation (WC) on PharmaCompass.
Eprosartan Active pharmaceutical ingredient (API) is produced in GMP-certified manufacturing facility.
GMP stands for Good Manufacturing Practices, which is a system used in the pharmaceutical industry to make sure that goods are regularly produced and monitored in accordance with quality standards. The FDA’s current Good Manufacturing Practices requirements are referred to as cGMP or current GMP which indicates that the company follows the most recent GMP specifications. The World Health Organization (WHO) has its own set of GMP guidelines, called the WHO GMP. Different countries can also set their own guidelines for GMP like China (Chinese GMP) or the EU (EU GMP).
PharmaCompass offers a list of Eprosartan GMP manufacturers, exporters & distributors, which can be sorted by USDMF, JDMF, KDMF, CEP (COS), WC, API price, and more, enabling you to easily find the right Eprosartan GMP manufacturer or Eprosartan GMP API supplier for your needs.
A Eprosartan CoA (Certificate of Analysis) is a formal document that attests to Eprosartan's compliance with Eprosartan specifications and serves as a tool for batch-level quality control.
Eprosartan CoA mostly includes findings from lab analyses of a specific batch. For each Eprosartan CoA document that a company creates, the USFDA specifies specific requirements, such as supplier information, material identification, transportation data, evidence of conformity and signature data.
Eprosartan may be tested according to a variety of international standards, such as European Pharmacopoeia (Eprosartan EP), Eprosartan JP (Japanese Pharmacopeia) and the US Pharmacopoeia (Eprosartan USP).










