1. Acenocoumarin
2. Mini Sintrom
3. Mini-sintrom
4. Minisintrom
5. Nicoumalone
6. Sinkumar
7. Sinthrome
8. Sintrom
9. Syncoumar
10. Syncumar
11. Synthrom
1. Acenocoumarin
2. 152-72-7
3. Nicoumalone
4. Sintrom
5. Nitrovarfarian
6. Nitrowarfarin
7. Nicumalon
8. Sinthrome
9. Acenocumarol
10. Sinkumar
11. Syncoumar
12. Syncumar
13. Acenokumarin
14. Sincoumar
15. Sinthrom
16. Ascumar
17. Syntrom
18. Zotil
19. Acenocoumarolum
20. Acenocumarolo
21. Sintroma
22. Mini-sintrom
23. Nitrophenylacetylethyl-4-hydroxycoumarine
24. Acenocoumarolum [inn-latin]
25. Acitrom
26. Trombostop
27. Acenocoumarol [inn]
28. G-23350
29. 3-(alpha-acetonyl-4-nitrobenzyl)-4-hydroxycoumarin
30. G 23350
31. 3-(alpha-acetonyl-p-nitrobenzyl)-4-hydroxycoumarin
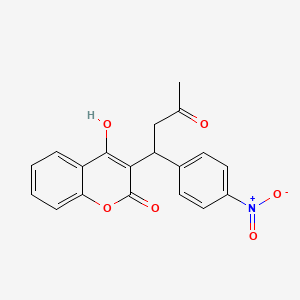
32. 4-hydroxy-3-(1-(4-nitrophenyl)-3-oxobutyl)-2h-1-benzopyran-2-one
33. 3-(alpha-p-nitrophenyl-beta-acetylethyl)-4-hydroxycoumarin
34. 4-hydroxy-3-[1-(4-nitrophenyl)-3-oxobutyl]chromen-2-one
35. 3-(alpha-(p-nitrophenol)-beta-acetylethyl)-4-hydroxycoumarin
36. 3-(alpha-(4'-nitrophenyl)-beta-acetylethyl)-4-hydroxycoumarin
37. Acenocoumarol (inn)
38. Neositron
39. 4-hydroxy-3-[1-(4-nitrophenyl)-3-oxobutyl]-2h-chromen-2-one
40. Nsc-760052
41. 2h-1-benzopyran-2-one, 4-hydroxy-3-(1-(4-nitrophenyl)-3-oxobutyl)-
42. Mls000539171
43. I6wp63u32h
44. Acenocumarolum
45. Chebi:53766
46. Minisintrom
47. Smr000162652
48. Acenokumarin [czech]
49. Acenocumarolo [dcit]
50. Dsstox_cid_2541
51. 3-(a-acetonyl-p-nitrobenzyl)-4-hydroxycoumarin
52. Dsstox_rid_76619
53. Dsstox_gsid_22541
54. 2h-1-benzopyran-2-one, 4-hydroxy-3-[1-(4-nitrophenyl)-3-oxobutyl]-
55. Mini-sintrom (tn)
56. Hsdb 3201
57. Einecs 205-807-3
58. G-23,350
59. Unii-i6wp63u32h
60. 4-hydroxy-3-(1-(4-nitrophenyl)-3-oxobutyl)-2h-chromen-2-one
61. Acenocoumarol [inn:ban:nf]
62. (+/-)-acenocoumarin
63. G23350
64. Ncgc00016414-01
65. Cas-152-72-7
66. Prestwick_773
67. Mfcd00137816
68. 1185071-64-0
69. Opera_id_1500
70. Prestwick0_000110
71. Prestwick1_000110
72. Prestwick2_000110
73. Prestwick3_000110
74. Acenocoumarol [mi]
75. Acenocoumarol [hsdb]
76. Schembl33543
77. Bspbio_000100
78. Ab-014/25000129
79. Mls001074461
80. Acenocoumarol [mart.]
81. 3-(alpha-acetonyl-p-nitrobenzyl)-4-hydroxy-coumarin
82. Spbio_002039
83. Acenocoumarol [who-dd]
84. Bpbio1_000110
85. Chembl397420
86. Gtpl9015
87. Schembl1477562
88. Coumarin, 3-(alpha-acetonyl-p-nitrobenzyl)-4-hydroxy-
89. Dtxsid2022541
90. Dtxsid00991186
91. Acenocoumarol, >=98% (hplc)
92. Hms1568e22
93. Hms2095e22
94. Hms2232p20
95. Hms3372j11
96. Hms3713f17
97. Pharmakon1600-01502411
98. Hy-b1014
99. Tox21_110430
100. Nsc760052
101. Akos015962123
102. Tox21_110430_1
103. Ab03786
104. Ab07575
105. Ab07577
106. Ccg-213077
107. Cs-4527
108. Db01418
109. Nsc 760052
110. Ncgc00179658-01
111. Ncgc00179658-04
112. As-56473
113. Ab00513804
114. Ft-0660959
115. Ft-0660960
116. Ft-0660961
117. D07064
118. T70324
119. Ab00513804_02
120. Ab00527557-09
121. 152a727
122. Q304088
123. Sr-01000678252
124. 2-acetamido-1,2,5-trideoxy-1,5-imino-d-glucitol
125. Sr-01000678252-3
126. W-108047
127. 3-(.alpha.-acetonyl-4-nitrobenzyl)-4-hydroxycoumarin
128. 3-(.alpha.-acetonyl-p-nitrophenyl)-4-hydroxycoumarin
129. Brd-a65051990-001-03-8
130. 3-(.alpha.-acetonyl-p-nitrobenzyl)-4-hydroxy-coumarin
131. Coumarin, 3-(.alpha.-acetonyl-p-nitrobenzyl)-4-hydroxy-
132. 3-(.alpha.-acetonyl-p-nitrobenzyl)-4-hydroxycoumarin
133. 3-(.alpha.-p-nitrophenyl-.beta.-acetylethyl)-4-hydroxycoumarin
134. 2-hydroxy-3-[1-(4-nitrophenyl)-3-oxobutyl]-4h-1-benzopyran-4-one
135. 3-(.alpha.-(4-nitrophenyl)-.beta.-acetylethyl)-4-hydroxycoumarin
136. 3-(.alpha.-(p-nitrophenol)-.beta.-acetylethyl)-4-hydroxycoumarin
137. 4-hydroxy-3-[1-(4-nitrophenyl)-3-oxobutyl]-2h-chromen-2-one #
138. Acenocoumarol, United States Pharmacopeia (usp) Reference Standard
| Molecular Weight | 353.3 g/mol |
|---|---|
| Molecular Formula | C19H15NO6 |
| XLogP3 | 2.5 |
| Hydrogen Bond Donor Count | 1 |
| Hydrogen Bond Acceptor Count | 6 |
| Rotatable Bond Count | 4 |
| Exact Mass | 353.08993720 g/mol |
| Monoisotopic Mass | 353.08993720 g/mol |
| Topological Polar Surface Area | 109 Ų |
| Heavy Atom Count | 26 |
| Formal Charge | 0 |
| Complexity | 614 |
| Isotope Atom Count | 0 |
| Defined Atom Stereocenter Count | 0 |
| Undefined Atom Stereocenter Count | 1 |
| Defined Bond Stereocenter Count | 0 |
| Undefined Bond Stereocenter Count | 0 |
| Covalently Bonded Unit Count | 1 |
Anticoagulants
National Library of Medicine's Medical Subject Headings online file (MeSH, 1999)
ACTIONS & USES OF ACENOCOUMAROL ARE THOSE OF DICOUMAROL. ... DRUG INTERACTIONS ARE SAME AS THOSE OF DICOUMAROL.
Osol, A. and J.E. Hoover, et al. (eds.). Remington's Pharmaceutical Sciences. 15th ed. Easton, Pennsylvania: Mack Publishing Co., 1975., p. 73
ACENOCOUMAROL IS MOST POTENT OF PROTHROMBOPENIC ANTICOAGULANTS.
Osol, A. and J.E. Hoover, et al. (eds.). Remington's Pharmaceutical Sciences. 15th ed. Easton, Pennsylvania: Mack Publishing Co., 1975., p. 763
In a randomized double blind study the efficacy and safety of continuous iv heparin plus acenocoumarol ... were compared with the efficacy and safety of acenocoumarol alone in the treatment of proximal vein thrombosis in 120 patients who were randomly assigned to receive heparin by continuous iv infusion for a minimum of 7 days plus acenocoumarol or an identical infusion of placebo acenocoumarol. Each patient was followed for 6 months . The study was terminated early in the group that received acenocoumarol alone because of an excess of symptomatic events (20% as compared with 6.7% in the combined therapy group). Asymptomatic extension of venous thrombosis was observed in 39.6% of the patients in the acenocoumarol group and in 8.2% of patients treated with heparin plus acenocoumarol. Major bleeding complications were infrequent and comparable in the 2 groups. It was concluded that patients with proximal vein thrombosis require initial treatment with full dose heparin, which can safely be combined with acenocoumarol therapy.
PMID:1406880 Brandjes DPN et al; New Eng J Med 327: 1485-9 (1992)
For more Therapeutic Uses (Complete) data for ACENOCOUMAROL (14 total), please visit the HSDB record page.
Contraindications to oral anticoagulants include pre-existing or coexisting abnormalities of blood coagulation, active bleeding, recent or imminent surgery of the central nervous system or eye, diagnostic or therapeutic procedures with potential for uncontrollable bleeding including lumbar puncture, malignant hypertension, peptic ulceration, pregnancy, threatened abortion, intrauterine device, cerebrovascular hemorrhage, and bacterial endocarditis. Relative contraindications include thrombocytopenia, pericarditis, pericardial effusions, and unreliability of the patient or of patient supervision. /Oral anticoagulants/
Haddad, L.M., Clinical Management of Poisoning and Drug Overdose. 2nd ed. Philadelphia, PA: W.B. Saunders Co., 1990., p. 308
Most commonly, oral anticoagulant-induced bleeding is minor and consists of bruising, hematuria, epistaxis, conjunctival hemorrhage, minor gastrointestinal bleeding, bleeding from wounds and sites of trauma, and vaginal bleeding. More serious major or fatal bleeding is most commonly gastrointestinal, intracranial, vaginal, retroperitoneal, or related to a wound or site of trauma, although a large variety of other sites of bleeding have been reported. Intracranial bleeding occurs most frequently in patients receiving oral anticoagulants for cerebrovascular disease and most commonly presents as a subdural hematoma, often unassociated with head trauma. Fatal gastrointestinal bleeding is most commonly from a peptic ulcer, although any gastrointestinal lesion may be a potential source of major bleeding. Overall, a bleeding lesion can be identified in about two thirds of cases of oral anticoagulants-related hemorrhage. /Oral anticoagulants/
Haddad, L.M., Clinical Management of Poisoning and Drug Overdose. 2nd ed. Philadelphia, PA: W.B. Saunders Co., 1990., p. 311
Overall, the bleeding rate of oral anticoagulant therapy is influenced by several factors: the intensity of anticoagulation, either intentionally or inadvertent; the underlying clinical disorder for which anticoagulant therapy is used (with bleeding occurring most frequently in ischemic cerebrovascular disease and venous thromboembolism; and, with bleeding occurring most commonly in the elderly; the presence of adverse drug interactions or comorbid factors such as clinical states potentiating warfarin action, pre-existing hemorrhagic diathesis, malignancy, recent surgery, trauma, or pre-existing potential bleeding sites (e.g., surgical wound, peptic ulcer, recent cerebral hemorrhage, carcinoma of colon); the simultaneous use of aspirin (but not of dipyridamole); and patient reliability (e.g., increased bleeding in alcoholics not due to ethanol-warfarin drug interaction but rather to unreliability of drug intake). /Oral anticoagulants/
Haddad, L.M., Clinical Management of Poisoning and Drug Overdose. 2nd ed. Philadelphia, PA: W.B. Saunders Co., 1990., p. 310
OF COUMARIN DERIVATIVES, ACENOCOUMAROL...CONTAINS NITROBENZENE MOIETY & MAY BE POTENTIALLY DANGEROUS FOR LONG-TERM USE.
American Medical Association, AMA Department of Drugs, AMA Drug Evaluations. 3rd ed. Littleton, Massachusetts: PSG Publishing Co., Inc., 1977., p. 115
For more Drug Warnings (Complete) data for ACENOCOUMAROL (28 total), please visit the HSDB record page.
For the treatment and prevention of thromboembolic diseases. More specifically, it is indicated for the prevention of cerebral embolism, deep vein thrombosis, pulmonary embolism, thromboembolism in infarction and transient ischemic attacks. It is used for the treatment of deep vein thrombosis and myocardial infarction.
Acenocoumarol inhibits the reduction of vitamin K by vitamin K reductase. This prevents carboxylation of certain glutamic acid residues near the N-terminals of clotting factors II, VII, IX and X, the vitamin K-dependent clotting factors. Glutamic acid carboxylation is important for the interaction between these clotting factors and calcium. Without this interaction, clotting cannot occur. Both the extrinsic (via factors VII, X and II) and intrinsic (via factors IX, X and II) are affected by acenocoumarol.
Anticoagulants
Agents that prevent BLOOD CLOTTING. (See all compounds classified as Anticoagulants.)
B01AA07
S76 | LUXPHARMA | Pharmaceuticals Marketed in Luxembourg | Pharmaceuticals marketed in Luxembourg, as published by d'Gesondheetskeess (CNS, la caisse nationale de sante, www.cns.lu), mapped by name to structures using CompTox by R. Singh et al. (in prep.). List downloaded from https://cns.public.lu/en/legislations/textes-coordonnes/liste-med-comm.html. Dataset DOI:10.5281/zenodo.4587355
B - Blood and blood forming organs
B01 - Antithrombotic agents
B01A - Antithrombotic agents
B01AA - Vitamin k antagonists
B01AA07 - Acenocoumarol
Absorption
Rapidly absorbed orally with greater than 60% bioavailability. Peak plasma levels are attained 1 to 3 hours following oral administration.
Route of Elimination
Mostly via the kidney as metabolites
Volume of Distribution
The volume of distribution at steady-state appeared to be significantly dose dependent: 78 ml/kg for doses < or = 20 microg/kg and 88 ml/kg for doses > 20 microg/kg respectively
ACENOCOUMAROL IS LARGELY EXCRETED BY KIDNEYS, IN UNCHANGED FORM.
Goodman, L.S., and A. Gilman. (eds.) The Pharmacological Basis of Therapeutics. 5th ed. New York: Macmillan Publishing Co., Inc., 1975., p. 1362
Rats received sc 1 mg doses of the R- or S-enantiomers of acenocoumarol and biliary and urinary excretion patterns were studied. In 24 hr, 50% biliary and 20% urinary excretion was observed with no gross differences in metabolic pattern or amount of metabolites. Slight differences due to stereochemistry are /noted/.
PMID:2888860 Thussen HH, Baars LG; J Pharm Pharmacol 39: 655-7 (1987)
Extensively metabolized in the liver via oxidation forming two hydroxy metabolites and keto reduction producing two alcohol metabolites. Reduction of the nitro group produces an amino metabolite which is further transformed to an acetoamido metabolite. Metabolites do not appear to be pharmacologically active.
8 to 11 hours.
8 to 11 hours.
MICROMEDEX Thomson Health Care. USPDI - Drug Information for the Health Care Professional. 22nd ed. Volume 1. MICROMEDEX Thomson Health Care, Greenwood Village, CO. 2002. Content Reviewed and Approved by the U.S. Pharmacopeial Convention, Inc., p. 266
Acenocoumarol has a short half-life of 10 to 24 hours.
Hardman, J.G., L.E. Limbird, P.B., A.G. Gilman. Goodman and Gilman's The Pharmacological Basis of Therapeutics. 10th ed. New York, NY: McGraw-Hill, 2001., p. 1531
Acenocoumarol inhibits vitamin K reductase, resulting in depletion of the reduced form of vitamin K (vitamin KH2). As vitamin K is a cofactor for the carboxylation of glutamate residues on the N-terminal regions of vitamin K-dependent clotting factors, this limits the gamma-carboxylation and subsequent activation of the vitamin K-dependent coagulant proteins. The synthesis of vitamin K-dependent coagulation factors II, VII, IX, and X and anticoagulant proteins C and S is inhibited resulting in decreased prothrombin levels and a decrease in the amount of thrombin generated and bound to fibrin. This reduces the thrombogenicity of clots.
The oral anticoagulants block the regeneration of reduced vitamin K and thereby induce a state of functional vitamin K deficiency. The mechanism of the inhibition of reductase(s) by the coumarin drugs is not known. There exist reductases that are less sensitive to these drugs but that act only at relatively high concentrations of oxidized vitamin K; this property may explain the observation that administration of sufficient vitamin K can counteract even large doses of oral anticoagulants. /Oral Anticoagulants/
Hardman, J.G., L.E. Limbird, P.B., A.G. Gilman. Goodman and Gilman's The Pharmacological Basis of Therapeutics. 10th ed. New York, NY: McGraw-Hill, 2001., p. 1527
Both 4-hydroxycoumarin derivatives and indandiones (also known as oral anticoagulants) are antagonists of vitamin K. Their use as rodenticides is based on the inhibition of the vitamin K-dependent step in the synthesis of a number of blood coagulation factors. The vitamin K-dependent proteins ...in the coagulation cascade... are the procoagulant factors II (prothrombin), VII (proconvertin), IX (Christmas factor) and X (Stuart-Prower factor), and the coagulation-inhibiting proteins C and S. All these proteins are synthesized in the liver. Before they are released into the circulation the various precursor proteins undergo substantial (intracellular) post-translational modification. Vitamin K functions as a co-enzyme in one of these modifications, namely the carboxylation at well-defined positions of 10-12 glutamate residues into gamma-carboxyglutamate (Gla). The presence of these Gla residues is essential for the procoagulant activity of the various coagulations factors. Vitamin K hydroquinone (KH2) is the active co-enzyme, and its oxidation to vitamin K 2,3-epoxide (KO) provides the energy required for the carboxylation reaction. The epoxide is than recycled in two reduction steps mediated by the enzyme KO reductase... . The latter enzyme is the target enzyme for coumarin anticoagulants. Their blocking of the KO reductase leads to a rapid exhaustion of the supply of KH2, and thus to an effective prevention of the formation of Gla residues. This leads to an accumulation of non-carboxylated coagulation factor precursors in the liver. In some cases these precursors are processed further without being carboxylated, and (depending on the species) may appear in the circulation. At that stage the under-carboxylated proteins are designated as descarboxy coagulation factors. Normal coagulation factors circulate in the form of zymogens, which can only participate in the coagulation cascade after being activated by limited proteolytic degradation. Descarboxy coagulation factors have no procoagulant activity (i.e. they cannot be activated) and neither they can be converted into the active zymogens by vitamin K action. Whereas in anticoagulated humans high levels of circulating descarboxy coagulation factors are detectable, these levels are negligible in warfarin-treated rats and mice. /Anticoagulant rodenticides/
WHO; Environ Health Criteria 175: Anticoagulant Rodenticides p.46 (1995)