1. Benazapril
2. Benazepril Hydrochloride
3. Benzazepril
4. Briem
5. Cgs-14824-a
6. Cgs-14824a
7. Cibacne
8. Cibacen
9. Labopal
10. Lotensin
1. 86541-75-5
2. Benazeprilum [latin]
3. Benazeprilum
4. Lotrel
5. Benazepril Sandoz
6. Cgs-14824a
7. Forteekor
8. Cibacen Ws
9. Benazepril (inn)
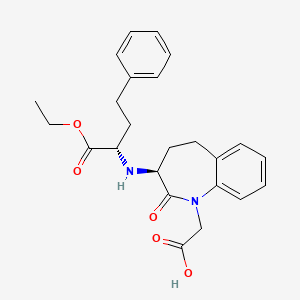
10. 2-[(3s)-3-[[(2s)-1-ethoxy-1-oxo-4-phenylbutan-2-yl]amino]-2-oxo-4,5-dihydro-3h-1-benzazepin-1-yl]acetic Acid
11. C09aa07
12. Udm7q7qwp8
13. Chembl838
14. Chebi:3011
15. 1h-1-benzazepine-1-acetic Acid, 3-((1-(ethoxycarbonyl)-3-phenylpropyl)amino)-2,3,4,5-tetrahydro-2-oxo-, (s-(r*,r*))-
16. [(3s)-3-{[(1s)-1-(ethoxycarbonyl)-3-phenylpropyl]amino}-2-oxo-2,3,4,5-tetrahydro-1h-1-benzazepin-1-yl]acetic Acid
17. 109010-10-8
18. Benazepril [inn]
19. Benazepril [inn:ban]
20. Cgs-14824-a
21. Benazepril Free Base
22. [(3s)-3-{[(2s)-1-ethoxy-1-oxo-4-phenylbutan-2-yl]amino}-2-oxo-2,3,4,5-tetrahydro-1h-1-benzazepin-1-yl]acetic Acid
23. 2-((s)-3-(((s)-1-ethoxy-1-oxo-4-phenylbutan-2-yl)amino)-2-oxo-2,3,4,5-tetrahydro-1h-benzo[b]azepin-1-yl)acetic Acid
24. 2-[(3s)-3-{[(2s)-1-ethoxy-1-oxo-4-phenylbutan-2-yl]amino}-2-oxo-2,3,4,5-tetrahydro-1h-1-benzazepin-1-yl]acetic Acid
25. Benazepril Sandoz (tn)
26. Unii-udm7q7qwp8
27. Forteekor [veterinary] (tn)
28. ((3s)-3-(((1s)-1-(ethoxycarbonyl)-3-phenylpropyl)amino)-2-oxo-2,3,4,5-tetrahydro-1h-1-benzazepin-1-yl)acetic Acid
29. 1h-1-benzazepine-1-acetic Acid, 3-(((1s)-1-(ethoxycarbonyl)-3-phenylpropyl)amino)-2,3,4,5-tetrahydro-2-oxo-, (3s)-
30. 1h-1-benzazepine-1-acetic Acid, 3-[[(1s)-1-(ethoxycarbonyl)-3-phenylpropyl]amino]-2,3,4,5-tetrahydro-2-oxo-, (3s)-
31. Benazepril Impurity A
32. Spectrum_001922
33. Benazepril [mi]
34. Spectrum2_000482
35. Spectrum3_001674
36. Spectrum4_000286
37. Spectrum5_001546
38. Benazepril [vandf]
39. Benazepril [who-dd]
40. Schembl16396
41. Bspbio_003487
42. Kbiogr_000812
43. Kbioss_002464
44. Mls006011854
45. Bidd:gt0800
46. Spbio_000343
47. Gtpl6374
48. Dtxsid5022645
49. Hsdb 7081
50. Kbio2_002457
51. Kbio2_005025
52. Kbio2_007593
53. Kbio3_002707
54. Bcp12672
55. Hy-b0093
56. Zinc3781943
57. Bbl034011
58. Bdbm50021153
59. Mfcd00864466
60. S5938
61. Stk627447
62. Akos005560204
63. Cs-1795
64. Db00542
65. Benazepril [ema Epar Veterinary]
66. Ncgc00165740-01
67. Ncgc00165740-02
68. Ncgc00165740-03
69. Ncgc00165740-04
70. [(3s)-3-({(1s)-1-[(ethyloxy)carbonyl]-3-phenylpropyl}amino)-2-oxo-2,3,4,5-tetrahydro-1h-1-benzazepin-1-yl]acetic Acid
71. Smr000857173
72. Sbi-0206744.p001
73. C06843
74. D07499
75. Ab00698518-07
76. Ab00698518_08
77. Ab00698518_09
78. 541b744
79. A841713
80. Q592802
81. Brd-k49807096-003-02-3
82. Tert Butyl-3-(3s) Amino-2,3,4,5-tetrahydro-1h(1) Benzazepin-2-one-1-acetate
83. Tert Butyl-3-(3s)amino-2,3,4,5-tetrahydro-1h(1)benzazepin-2-one-1-acetate
84. 2-((s)-3-((s)-1-ethoxy-1-oxo-4-phenylbutan-2-ylamino)-2-oxo-2,3,4,5-tetrahydro-1h-benzo[b]azepin-1-yl)acetic Acid
85. 2-[(3s)-3-[[(1s)-1-ethoxycarbonyl-3-phenyl-propyl]amino]-2-oxo-4,5-dihydro-3h-1-benzazepin-1-yl]acetic Acid;benazepril
86. 2-[(4s)-4-[[(1s)-1-ethoxycarbonyl-3-phenyl-propyl]amino]-3-oxo-2-azabicyclo[5.4.0]undeca-7,9,11-trien-2-yl]acetic Acid
1. 86541-78-8
2. Benazeprilate
3. Benazeprilat
| Molecular Weight | 424.5 g/mol |
|---|---|
| Molecular Formula | C24H28N2O5 |
| XLogP3 | 1.3 |
| Hydrogen Bond Donor Count | 2 |
| Hydrogen Bond Acceptor Count | 6 |
| Rotatable Bond Count | 10 |
| Exact Mass | 424.19982200 g/mol |
| Monoisotopic Mass | 424.19982200 g/mol |
| Topological Polar Surface Area | 95.9 Ų |
| Heavy Atom Count | 31 |
| Formal Charge | 0 |
| Complexity | 619 |
| Isotope Atom Count | 0 |
| Defined Atom Stereocenter Count | 2 |
| Undefined Atom Stereocenter Count | 0 |
| Defined Bond Stereocenter Count | 0 |
| Undefined Bond Stereocenter Count | 0 |
| Covalently Bonded Unit Count | 1 |
/CLINICAL TRIALS/ ClinicalTrials.gov is a registry and results database of publicly and privately supported clinical studies of human participants conducted around the world. The Web site is maintained by the National Library of Medicine (NLM) and the National Institutes of Health (NIH). Each ClinicalTrials.gov record presents summary information about a study protocol and includes the following: Disease or condition; Intervention (for example, the medical product, behavior, or procedure being studied); Title, description, and design of the study; Requirements for participation (eligibility criteria); Locations where the study is being conducted; Contact information for the study locations; and Links to relevant information on other health Web sites, such as NLM's MedlinePlus for patient health information and PubMed for citations and abstracts for scholarly articles in the field of medicine. Benazepril is included in the database.
NIH/NLM; ClinicalTrials.Gov. Available from, as of August 30, 2017: https://clinicaltrials.gov/
Lotensin is indicated for the treatment of hypertension, to lower blood pressure. Lowering blood pressure reduces the risk of fatal and nonfatal cardiovascular events, primarily strokes and myocardial infarctions. ... It may be used alone or in combination with thiazide diuretics. /Included in US product label/
NIH; DailyMed. Current Medication Information for Lotensin (Benazepril Hydrochloride Tablet) (Updated: August 2017). Available from, as of November 2, 2017: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=2abb091b-a53e-46b0-9b84-e5ee8f2bdd8e
ACE inhibitors have been used in the management of heart failure, usually in conjunction with other agents such as cardiac glycosides, diuretics, and beta-blockers. /Angiotensin-converting enzyme (ACE) inhibitors; NOT included in US product label/
American Society of Health-System Pharmacists 2017; Drug Information 2017. Bethesda, MD. 2017, p. 2067
Both angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor antagonists have been shown to slow the rate of progression of renal disease in patients with diabetes mellitus and persistent albuminuria, and use of a drug from either class is recommended in such patients with modestly elevated (30-300 mg/24 hours) or higher (exceeding 300 mg/24 hours) levels of urinary albumin excretion. The usual precautions of ACE inhibitor or angiotensin II receptor antagonist therapy in patients with substantial renal impairment should be observed. /Angiotensin-converting enzyme (ACE) inhibitors; NOT included in US product label/
American Society of Health-System Pharmacists 2017; Drug Information 2017. Bethesda, MD. 2017, p. 2067
For more Therapeutic Uses (Complete) data for Benazepril (7 total), please visit the HSDB record page.
/BOXED WARNING/ When pregnancy is detected, discontinue Lotensin as soon as possible. Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus.
NIH; DailyMed. Current Medication Information for Lotensin (Benazepril Hydrochloride Tablet) (Updated: August 2017). Available from, as of November 2, 2017: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=2abb091b-a53e-46b0-9b84-e5ee8f2bdd8e
Rare angiotensin-converting enzyme (ACE) inhibitor-associated clinical syndrome manifested initially by cholestatic jaundice; may progress to fulminant hepatic necrosis and is potentially fatal. Patients receiving an ACE inhibitor, including benazepril, who develop jaundice or marked elevations of hepatic enzymes should discontinue the drug and receive appropriate monitoring.
American Society of Health-System Pharmacists 2017; Drug Information 2017. Bethesda, MD. 2017, p. 2068
Serum potassium should be monitored periodically in patients receiving Lotensin. Drugs that inhibit the renin-angiotensin system can cause hyperkalemia. Risk factors for the development of hyperkalemia include renal insufficiency, diabetes mellitus, and the concomitant use of potassium-sparing diuretics, potassium supplements and/or potassium-containing salt substitutes.
NIH; DailyMed. Current Medication Information for Lotensin (Benazepril Hydrochloride Tablet) (Updated: August 2017). Available from, as of November 2, 2017: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=2abb091b-a53e-46b0-9b84-e5ee8f2bdd8e
Adverse effects reported in greater than 1% of patients receiving benazepril include headache, dizziness, fatigue, somnolence, postural dizziness, nausea, and cough. Adverse effects reported in greater than 1% of patients receiving benazepril in fixed combination with hydrochlorothiazide include dizziness, fatigue, postural dizziness, headache, cough, hypertonia, vertigo, nausea, impotence, and somnolence. Adverse effects reported in greater than 1% of patients receiving benazepril in fixed combination with amlodipine include cough, headache, dizziness, and edema.
American Society of Health-System Pharmacists 2017; Drug Information 2017. Bethesda, MD. 2017, p. 2069
For more Drug Warnings (Complete) data for Benazepril (16 total), please visit the HSDB record page.
Benazepril is indicated for the treatment of hypertension. It may be used alone or in combination with thiazide diuretics.
FDA Label
Benazepril, an angiotensin-converting enzyme (ACE) inhibitor, is a prodrug which, when hydrolyzed by esterases to its active Benazeprilat, is used to treat hypertension and heart failure, to reduce proteinuria and renal disease in patients with nephropathies, and to prevent stroke, myocardial infarction, and cardiac death in high-risk patients. Benazepril and Benazeprilat inhibit angiotensin-converting enzyme (ACE) in human subjects and animals. ACE is a peptidyl dipeptidase that catalyzes the conversion of angiotensin I to the vasoconstrictor substance, angiotensin II. Angiotensin II also stimulates aldosterone secretion by the adrenal cortex.
Antihypertensive Agents
Drugs used in the treatment of acute or chronic vascular HYPERTENSION regardless of pharmacological mechanism. Among the antihypertensive agents are DIURETICS; (especially DIURETICS, THIAZIDE); ADRENERGIC BETA-ANTAGONISTS; ADRENERGIC ALPHA-ANTAGONISTS; ANGIOTENSIN-CONVERTING ENZYME INHIBITORS; CALCIUM CHANNEL BLOCKERS; GANGLIONIC BLOCKERS; and VASODILATOR AGENTS. (See all compounds classified as Antihypertensive Agents.)
Angiotensin-Converting Enzyme Inhibitors
A class of drugs whose main indications are the treatment of hypertension and heart failure. They exert their hemodynamic effect mainly by inhibiting the renin-angiotensin system. They also modulate sympathetic nervous system activity and increase prostaglandin synthesis. They cause mainly vasodilation and mild natriuresis without affecting heart rate and contractility. (See all compounds classified as Angiotensin-Converting Enzyme Inhibitors.)
C09AA07
S76 | LUXPHARMA | Pharmaceuticals Marketed in Luxembourg | Pharmaceuticals marketed in Luxembourg, as published by d'Gesondheetskeess (CNS, la caisse nationale de sante, www.cns.lu), mapped by name to structures using CompTox by R. Singh et al. (in prep.). List downloaded from https://cns.public.lu/en/legislations/textes-coordonnes/liste-med-comm.html. Dataset DOI:10.5281/zenodo.4587355
C - Cardiovascular system
C09 - Agents acting on the renin-angiotensin system
C09A - Ace inhibitors, plain
C09AA - Ace inhibitors, plain
C09AA07 - Benazepril
Absorption
Bioavailability of oral dosing is 3% to 4% in horses. In humans at least 37% of oral benazepril is absorbed and reaches peak plasma concentration in 0.5 hours to 1 hour. Other studies have shown a peak plasma concentration at a median of 1.5 hours.
Route of Elimination
Benazepril and benazeprilat are cleared predominantly by renal excretion in healthy subjects with normal renal function. Nonrenal (i.e., biliary) excretion accounts for approximately 11%-12% of benazeprilat excretion in healthy subjects.
Volume of Distribution
The final population pharmacokinetic model in one study estimated the volume of distribution to be 20369.9L.
Clearance
The final population pharmacokinetic model of one study estimates the clearance to be 12930.0L.
/MILK/ Minimal amounts of unchanged benazepril and of benazeprilat are excreted into the breast milk of lactating women treated with benazepril. A newborn child ingesting entirely breast milk would receive less than 0.1% of the mg/kg maternal dose of benazepril and benazeprilat.
NIH; DailyMed. Current Medication Information for Lotensin (Benazepril Hydrochloride Tablet) (Updated: August 2017). Available from, as of November 2, 2017: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=2abb091b-a53e-46b0-9b84-e5ee8f2bdd8e
Benazepril and benazeprilat are cleared predominantly by renal excretion. About 37% of an orally administered dose was recovered in urine as benazeprilat (20%), benazeprilat glucuronide (8%), benazepril glucuronide (4%) and as trace amounts of benazepril. Nonrenal (i.e., biliary) excretion accounts for approximately 11% - 12% of benazeprilat excretion. The effective half-life of benazeprilat following once daily repeat oral administration of benazepril hydrochloride is 10 to 11 hours. Thus, steady-state concentrations of benazeprilat should be reached after 2 or 3 doses of benazepril hydrochloride given once daily. Accumulation ratio based on AUC of benazeprilat was 1.19 following once daily administration.
NIH; DailyMed. Current Medication Information for Lotensin (Benazepril Hydrochloride Tablet) (Updated: August 2017). Available from, as of November 2, 2017: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=2abb091b-a53e-46b0-9b84-e5ee8f2bdd8e
Cleavage of the ester group (primarily in the liver) converts benazepril to its active metabolite, benazeprilat. Benazepril and benazeprilat are conjugated to glucuronic acid prior to urinary excretion.
Benazepril and benazeprilat are cleared predominantly by renal excretion. About 37% of an orally administered dose was recovered in urine as benazeprilat (20%), benazeprilat glucuronide (8%), benazepril glucuronide (4%) and as trace amounts of benazepril. Nonrenal (i.e., biliary) excretion accounts for approximately 11% - 12% of benazeprilat excretion. The effective half-life of benazeprilat following once daily repeat oral administration of benazepril hydrochloride is 10 to 11 hours. Thus, steady-state concentrations of benazeprilat should be reached after 2 or 3 doses of benazepril hydrochloride given once daily. Accumulation ratio based on AUC of benazeprilat was 1.19 following once daily administration.
NIH; DailyMed. Current Medication Information for Lotensin (Benazepril Hydrochloride Tablet) (Updated: August 2017). Available from, as of November 2, 2017: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=2abb091b-a53e-46b0-9b84-e5ee8f2bdd8e
After oral dosing in healthy dogs, benazepril is rapidly absorbed and converted into the active metabolite benazeprilat with peak levels of benazeprilat occurring approximately 75 minutes after dosing.
Plumb D.C. Veterinary Drug Handbook. 8th ed. (pocket). Ames, IA: Wiley-Blackwell, 2015., p. 146
Benazepril is almost completely metabolized to benazeprilat by cleavage of the ester group (primarily in liver). Both benazepril and benazeprilat undergo glucuronidation.
NIH; DailyMed. Current Medication Information for Lotensin (Benazepril Hydrochloride Tablet) (Updated: August 2017). Available from, as of November 2, 2017: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=2abb091b-a53e-46b0-9b84-e5ee8f2bdd8e
The half life of the prodrug benazepril is 2.78.5h. The half life of the active metabolite benazeprilat is 22.39.2h The accumulation half life of benazepril is 10 to 11 hours.
The elimination half life of benazeprilat is approximately 3.5 hours in healthy dogs. /Benazeprilat/
Plumb D.C. Veterinary Drug Handbook. 8th ed. (pocket). Ames, IA: Wiley-Blackwell, 2015., p. 146
The effective half-life of benazeprilat following once daily repeat oral administration of benazepril hydrochloride is 10 to 11 hours. /Benazeprilat/
NIH; DailyMed. Current Medication Information for Lotensin (Benazepril Hydrochloride Tablet) (Updated: August 2017). Available from, as of November 2, 2017: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=2abb091b-a53e-46b0-9b84-e5ee8f2bdd8e
Benazeprilat, the active metabolite of Benazepril, competes with angiotensin I for binding at the angiotensin-converting enzyme, blocking the conversion of angiotensin I to angiotensin II. Inhibition of ACE results in decreased plasma angiotensin II. As angiotensin II is a vasoconstrictor and a negative-feedback mediator for renin activity, lower concentrations result in a decrease in blood pressure and stimulation of baroreceptor reflex mechanisms, which leads to decreased vasopressor activity and to decreased aldosterone secretion.